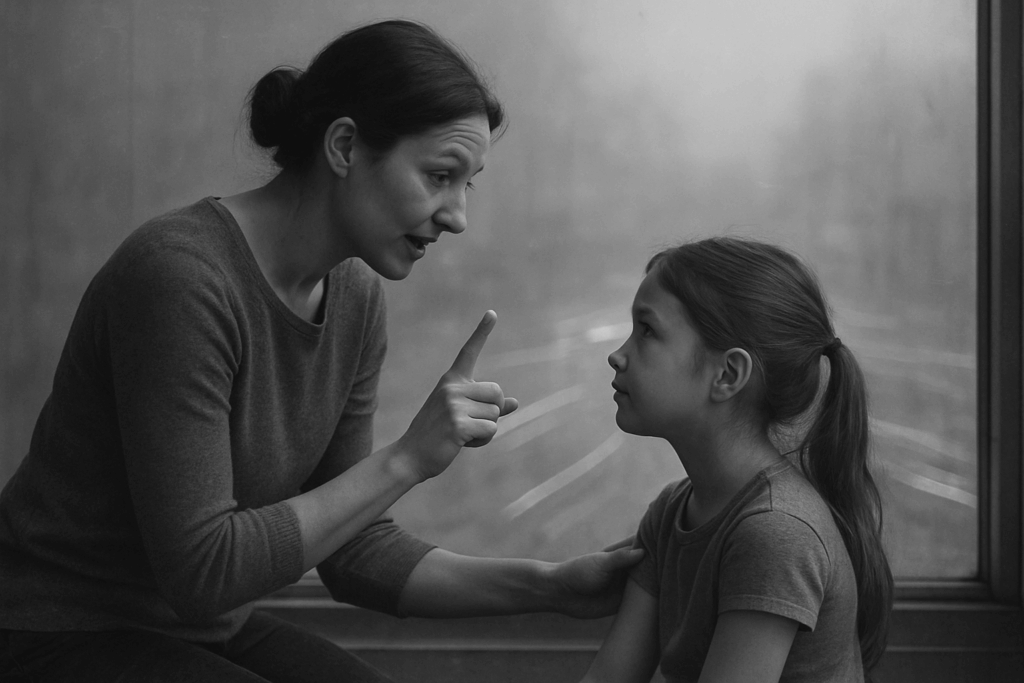
The morning starts the same way again. Backpack by the door. Shoes ready. And your teen, frozen on the edge of the bed, says they can’t go. Not won’t. Can’t. Maybe there are tears. Maybe there’s silence. Maybe a stomachache that feels real to them and unfamiliar to you.
You’ve tried the calm voice. The firm voice. The bargain. The early bedtime. And still, mornings keep collapsing in the same place.
What you’re seeing has a name, and it’s more common than most parents realize. When a teen consistently struggles to attend school because of overwhelming anxiety, dread, or emotional shutdown, clinicians often describe it as emotionally based school avoidance. It isn’t defiance. It isn’t laziness. It’s a signal that something underneath, often anxiety, depression, social fear, or burnout, has grown louder than your teen’s ability to push through it.
For families in smaller Arizona towns and rural communities, this can feel especially isolating. The nearest adolescent therapist might be two hours away. The school counselor is stretched thin. And the usual advice (“just get them to school”) starts to feel hollow when you’ve watched your kid melt down at the threshold.
What School Avoidance Actually Looks Like

It rarely arrives all at once. Most parents describe a slow drift.
Sunday nights get harder. Stomachaches show up before first period but disappear by lunchtime at home. Homework piles up. Friend group goes quiet. Your teen sleeps later, eats less at the table, and spends longer stretches in their room with the door closed.
Then come the bigger moments: the refusal to get in the car, the panic in the parking lot, the text from school saying they’re in the nurse’s office again.
Some teens shut down quietly. They go to school but stop participating, stop turning in work, stop talking to teachers. Others escalate, with crying, anger, or what looks like a panic attack at the front door. Both patterns matter. Both deserve attention.
Why Rural and Small-Town Families Face Extra Hurdles
Geography changes what’s possible. When you live an hour or more from a specialty clinic, weekly therapy can mean missed work, long drives, and a teen who’s already drained before the session begins.
School avoidance interventions in rural areas often hit the same walls: limited provider availability, fewer adolescent specialists, school staff trained mostly in academic supports rather than mental health response, and waitlists that stretch for months. Families end up patching together what they can, a school counselor here, a primary care visit there, while the underlying issue keeps growing.
This isn’t a parenting failure. It’s a resource gap. And it’s part of why virtual care has become a meaningful option for teens who need more than a once-a-week appointment but don’t need a hospital stay.
The Signals Worth Taking Seriously
Some school stress is part of growing up. A rough week, a hard test, a friendship that fell apart. Those usually pass.
The signs that suggest something deeper is going on tend to cluster and persist:
- Missing school more than one or two days per week for several weeks
- Physical symptoms (headaches, nausea, chest tightness) that fade outside of school hours
- Withdrawal from friends, activities, or family meals
- Sleep that’s flipped: awake at night, exhausted during the day
- Talk of feeling hopeless, trapped, “too much,” or a burden
- Self-harm, or any mention of not wanting to be here
- Sudden drops in grades from a teen who used to care
- Increased irritability, shutting down, or emotional flatness at home
If any signs of self-harm or suicidal thinking come up, treat that as urgent and reach out to a professional or crisis line the same day.
What Helps, and What “More Support” Can Mean
Many families start with what’s familiar: a check-in with the pediatrician, a meeting with the school counselor, maybe weekly outpatient therapy if it’s available. For some teens, that’s enough. For others, the avoidance keeps growing because the level of support doesn’t match the size of what they’re carrying.
When that happens, families sometimes hear about higher levels of care. One option that’s expanded significantly in recent years is the virtual intensive outpatient program, often called a virtual IOP. These programs typically meet several times a week for a few hours per session, online, with a mix of group therapy, individual sessions, and family work.
Research on telehealth IOPs for youth has shown meaningful symptom improvement across depression, anxiety, and suicidality (Evans-Chase et al., 2023; Gliske et al., 2022). Family involvement matters too. Teens whose caregivers participated in family therapy components stayed in treatment longer and engaged more fully (Berry et al., 2023). For LGBTQ+ teens, adapted telehealth IOPs have shown comparable or stronger improvement compared with standard groups (Berry et al., 2023).
The right fit depends on the teen. A virtual IOP isn’t a replacement for emergency care, and it isn’t the right level for every adolescent. But for a teen whose weekly therapy isn’t enough and whose life doesn’t allow a long drive to a clinic, it can bridge a real gap.
What Parents Can Do This Week
A few things tend to help while you’re figuring out the bigger picture.
Get curious before you get corrective. Instead of “Why won’t you go?” try “What part of the day feels hardest right now?” Teens often can’t name it cleanly, but the question itself lowers the temperature.
Loop in the school early. Ask about a 504 plan, modified attendance, or a re-entry plan. Most schools have more flexibility than parents realize, especially when a mental health concern is documented.
Talk to your teen’s pediatrician. A medical visit can rule out physical contributors (thyroid issues, sleep disorders, anemia) and open the door to a referral.
Keep mornings predictable, but lower the stakes on perfection. Getting to school late is better than not at all. A half day counts. Showing up to one class counts.
Watch your own bandwidth. Parenting a teen through this is exhausting, and your steadiness is part of the treatment. Sleep, support, and your own check-ins matter.
When to Reach for Something More
If avoidance has lasted more than a few weeks, if your teen’s mood is sliding, if weekly therapy isn’t moving the needle, or if you’re noticing safety concerns, that’s the point to ask a clinician about a higher level of care. Virtual options have made this more reachable for families outside major metro areas, with evening sessions, family components, and no long commute (Cherry et al., 2025).
You don’t have to wait until things hit a crisis to ask. Most programs offer a free consultation where you can describe what’s happening and get a sense of fit.
A Steadier Way Forward
School avoidance isn’t a character problem, and it isn’t something most teens can willpower their way out of. It’s a signal, often the loudest one a teen has, that they need more support than the current setup is offering.
The good news is that the options have grown. Rural families aren’t stuck with the same two choices they had a decade ago. Between school-based supports, telehealth therapy, and virtual intensive programs designed around family life, there’s more room now to match the level of care to what your teen is actually carrying.
What matters most is that someone noticed. You did.
Safety Disclaimer
If you or someone you love is in crisis, call 911 or go to the nearest emergency room. You can also call or text 988, or chat via 988lifeline.org to reach the Suicide & Crisis Lifeline. Support is free, confidential, and available 24/7.
Author Bio
Earl Wagner is a health content strategist focused on behavioural systems, clinical communication, and data-informed healthcare education.
Sources
- Michelle Evans-Chase. (2023). Understanding Treatment Needs of Youth in a Remote Intensive Outpatient Program Through Solicited Journals: Quality Improvement Analysis. JMIR formative research. https://doi.org/10.2196/45509
- Katie R Berry. (2023). The Impact of Family Therapy Participation on Youths and Young Adult Engagement and Retention in a Telehealth Intensive Outpatient Program: Quality Improvement Analysis. JMIR formative research. https://doi.org/10.2196/45305
- Katie R Berry. (2023). Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, Asexual, and Other Minoritized Gender and Sexual Identities-Adapted Telehealth Intensive Outpatient Program for Youth and Young Adults: Subgroup Analysis of Acuity and Improvement Following Treatment. JMIR formative research. https://doi.org/10.2196/45796
- Kate Gliske. (2022). Mental Health Outcomes for Youths With Public Versus Private Health Insurance Attending a Telehealth Intensive Outpatient Program: Quality Improvement Analysis. JMIR formative research. https://doi.org/10.2196/41721
















































































































































































































































































































































































































































































































































































































 Health & Wellness Contributor
Health & Wellness Contributor